

Flaws in Current Vaccine "Myth-Busting" Narratives: A Critical Review
How oversimplified "myth-busting" narratives is false vaccine safety

Overview of Current "Myth-Busting" Framework
Over the past two decades, public health institutions, medical organizations, and major media outlets have increasingly employed a "myth-busting" framework to respond to public concerns about vaccine safety.
A widely circulated table categorizes several common parental concerns about vaccines as "myths," offering brief rebuttals. See the following table from the paper Geoghegan 2020 “Vaccine Safety: Myths and Misinformation”:
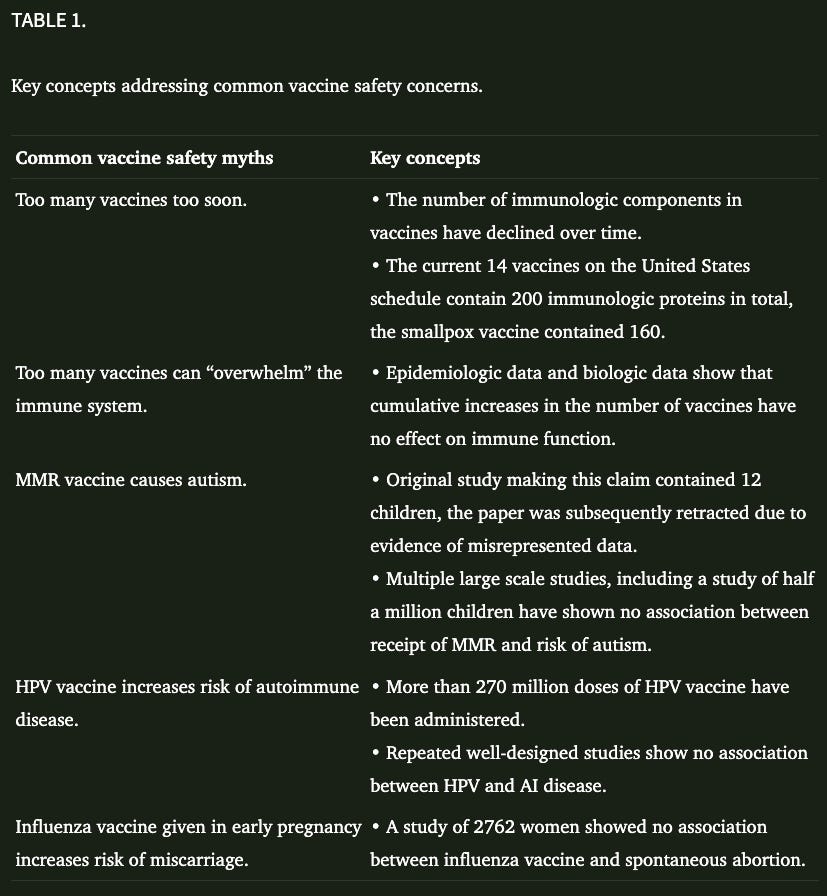
Labeling concerns as “myths” preemptively frames dissenters as irrational or misinformed rather than as engaged participants in a serious dialogue. Many of the so-called myths are not baseless conspiracy theories but nuanced hypotheses rooted in well-established biological principles such as immune development, toxicology, and systems biology.
Moreover, the myth-busting framework often simplifies multifaceted scientific issues into black-and-white claims, giving the illusion of certainty in areas where genuine scientific uncertainty or incompleteness persists.
By offering truncated rebuttals without acknowledging existing gaps, unresolved mechanisms, or conflicting data, the framework risks substituting public relations objectives for scientific rigor. This approach erodes trust, especially among scientifically literate audiences who recognize that real science rarely proceeds through blanket dismissals.
Finally, the myth-busting style of communication betrays an unscientific fear of inquiry. True science welcomes skepticism, values critical questioning, and evolves in response to new data. An intellectually honest public health apparatus would not merely "bust" concerns but would openly investigate them, refine hypotheses, and adapt public health policies as evidence demands.
In the sections that follow, we will critically examine several of the most prominent “vaccine myths” identified in this framework, and show how the current rebuttals fail to meet the ethical and scientific standards that the public deserves.
Key Gaps in the Arguments
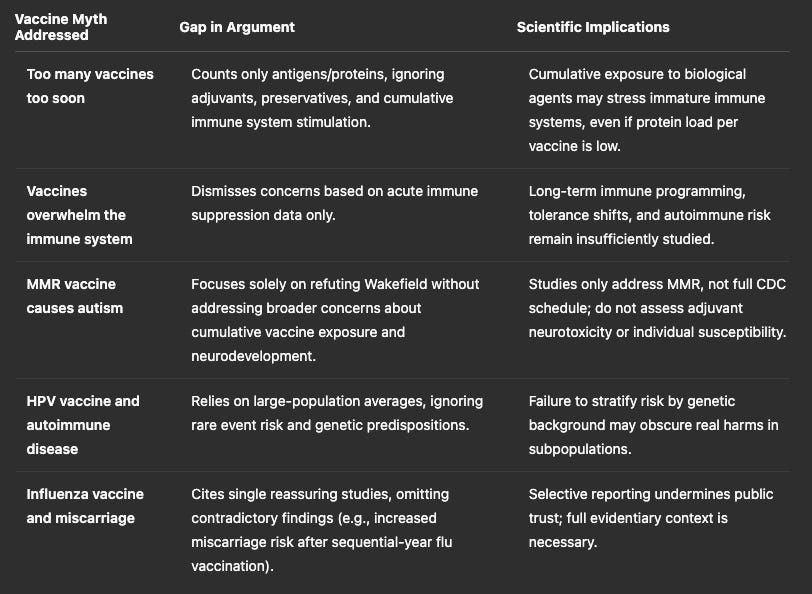
Myth 1: "Too many vaccines too soon"
The rebuttal often states that infants encounter more antigens daily through breathing and eating than from vaccines. However, this argument narrowly focuses on the number of immunogenic proteins, disregarding critical aspects such as adjuvants (e.g., aluminum compounds), preservatives, and stabilizers present in vaccines.
The immune system's burden is not limited to antigen exposure alone; cumulative exposure to synthetic additives, adjuvants, and repeated inflammatory triggers can have complex, poorly understood consequences, particularly during critical windows of immune and neurological development.
Scientifically, the absence of studies examining these cumulative effects leaves a significant safety gap.
Myth 2: "Vaccines overwhelm the immune system"
The typical counterargument cites that no immediate signs of immune suppression are observed following vaccination. However, this narrow view ignores the subtleties of immune programming.
Vaccines, by design, provoke an immune response, and frequent, repeated stimulation during infancy could theoretically alter immune regulatory mechanisms, tolerance thresholds, or inflammatory set-points later in life.
Emerging fields like immunometabolism and epigenetic immune imprinting suggest that early immune experiences can have lifelong impacts.
Without long-term, mechanistic studies into how vaccination patterns shape immune system development, sweeping assurances are scientifically premature.
Myth 3: "MMR vaccine causes autism"
Rebuttals to this concern usually focus on discrediting Andrew Wakefield's infamous 1998 study but this ignores the larger issue.
Most epidemiological studies investigate only the MMR vaccine—not the cumulative effect of multiple vaccines or the adjuvants contained within the overall childhood schedule.
Furthermore, genetic susceptibilities, mitochondrial dysfunction, and environmental toxin interactions with neurodevelopmental processes remain underexplored.
The scientific implication is clear: discrediting one paper does not resolve legitimate, mechanistic concerns about potential pathways linking immune activation and neurodevelopmental risks.
Myth 4: "HPV vaccine and autoimmune disease"
Counterarguments often point to large cohort studies that find no statistically significant increase in autoimmune disease rates following HPV vaccination.
However, these studies are typically underpowered to detect rare but serious adverse events and rarely stratify participants by genetic risk factors such as HLA type, which could predispose subsets of the population to autoimmune reactions.
Moreover, epidemiological averages can obscure critical harms that, while rare, are devastating at the individual level. Scientifically, failing to conduct subgroup analyses or mechanistic studies overlooks important safety signals and reinforces public skepticism.
Myth 5: "Influenza vaccine and miscarriage"
Proponents often cite studies showing no overall increase in miscarriage rates among vaccinated women. However, they frequently omit studies, such as the 2019 Donahue et al. study, which found an elevated risk of miscarriage associated with receiving influenza vaccines in two consecutive seasons.
Selectively citing reassuring studies without acknowledging conflicting data presents an incomplete and biased picture. Scientific integrity demands that all evidence—supportive and contradictory—be transparently discussed, especially when dealing with sensitive issues such as pregnancy and fetal health.
Broader Problems with the "Myth-Busting" Paradigm
There are larger problems here which we will examine in depth:
Conflation of Myth with Complex Hypothesis: Many so-called myths reflect nuanced, plausible scientific concerns deserving investigation.
Overreliance on Epidemiology: Lack of mechanistic toxicology studies creates blind spots regarding causality.
Neglect of Cumulative and Synergistic Effects: The effects of dozens of simultaneous exposures have not been adequately studied.
Framing Bias: The rhetorical strategy seeks to close debate, not advance understanding.
Neglect of Subpopulation Risks: Average risk is insufficient in public health ethics where identifiable vulnerable groups exist.
1. Conflation of Myth with Complex Hypothesis
Public health communications often label concerns about vaccines as “myths,” thereby dismissing them outright.
However, many so-called myths are not simple misunderstandings but reflect nuanced hypotheses that warrant serious scientific inquiry. For instance, questioning the cumulative effects of repeated immune stimulation in infancy is not a superstition; it is a plausible biological question rooted in immunology and developmental biology.
Conflating these concerns with conspiracy theories or ignorance delegitimizes sincere scientific and parental inquiry and risks alienating the very people institutions aim to persuade.
A truly scientific approach distinguishes between baseless rumors and legitimate hypotheses requiring open, ongoing investigation.
2. Overreliance on Epidemiology
Epidemiological studies are valuable for detecting broad trends across populations, but they are poorly suited for detecting mechanistic causes or rare but serious harms.
Most vaccine safety rebuttals rely heavily on epidemiology while ignoring mechanistic toxicology, immunology, and systems biology. This leaves major blind spots, such as understanding how adjuvants or repeated immune activations during critical developmental windows might subtly alter long-term neuroimmune health.
Without complementary mechanistic studies, epidemiological reassurance offers an incomplete picture and fails to detect complex, multifactorial harms that may only emerge under certain conditions or in vulnerable subgroups.
3. Neglect of Cumulative and Synergistic Effects
While vaccines are individually studied for safety, very few studies assess the combined effects of the full vaccine schedule or multiple simultaneous vaccinations.
This is a crucial oversight, because biological systems often respond differently to cumulative exposures than to isolated ones. Multiple immune challenges, adjuvants, and environmental toxins may have synergistic effects that are not captured in isolated single-product safety trials.
Ignoring cumulative and synergistic exposures violates a basic principle of toxicology: “the dose makes the poison” often depends on cumulative burden, not single events.
True vaccine safety science must rigorously assess cumulative biological stress over time.
4. Framing Bias
The rhetorical strategy often used in myth-busting tables and communications seeks to close debate rather than foster deeper understanding.
By labeling questions as myths and presenting rebuttals as final, these efforts project certainty where scientific uncertainty or complexity exists. This framing subtly pressures readers into a binary acceptance-or-rejection mindset and discourages legitimate skepticism.
It risks transforming science—which thrives on ongoing inquiry, revision, and falsifiability—into a dogmatic institution that cannot admit uncertainty or error.
In the long run, framing bias erodes public trust by making institutions appear more concerned with protecting orthodoxy than pursuing truth.
5. Neglect of Subpopulation Risks
Public health messaging typically presents risks and benefits averaged across large populations. While this approach works for broad policy, it is ethically inadequate when it comes to individual medical decisions.
Rare but severe vaccine injuries, for example, may not be statistically significant in population studies but are devastating at the personal level.
Moreover, individuals with specific genetic vulnerabilities, mitochondrial disorders, immune dysregulation, or previous adverse reactions face different risk profiles that are obscured in population-wide data.
Ethical medicine demands that such subpopulations be explicitly acknowledged, studied, and accommodated rather than marginalized or ignored for the sake of reassuring the majority.
Recommendations for Reform
The vaccine program in need of reform. To address the identified gaps, the following recommendations should be made.
1. Treat Vaccine Safety as an Ongoing Scientific Endeavor
Vaccine safety must be treated as a dynamic, evolving area of scientific inquiry—not a finished chapter. Science thrives on continual questioning, hypothesis-testing, and openness to updating conclusions when new evidence emerges.
Yet much of public health communication around vaccines presents safety as “settled” and beyond question. This attitude stifles necessary scientific vigilance and risks overlooking emerging risks, especially with changes in vaccine formulations, schedules, or adjuvant technologies.
An honest scientific culture must frame vaccine safety as a living research program requiring ongoing vigilance, refinement, and humility.
2. Mandate Transparent, Public Release of Clinical and Post-Market Data
Trust cannot be built on inaccessible or secretive data. Full, unredacted access to clinical trial data, adverse event reporting systems, and post-market surveillance information must be guaranteed to independent researchers and the public.
Only radical transparency can enable genuine external review, replication of analyses, and correction of errors or overlooked signals. Without access to raw data, independent science is impossible, and regulatory agencies risk becoming perceived as captive to the industries they regulate.
Transparency must become the default—not an exception—for all vaccine-related research.
3. Fund Mechanistic Studies on Adjuvants, Cumulative Exposure, and Long-Term Outcomes
Large epidemiological studies are necessary but insufficient. Mechanistic research—into how adjuvants, cumulative vaccine exposures, timing of vaccination relative to developmental milestones, and individual genetic factors influence immune and neurological development—must become a top funding priority.
Only through understanding biological pathways can we anticipate risks, stratify them among populations, and develop truly safer vaccines.
Funding should prioritize long-term studies that examine neurodevelopment, immune tolerance, mitochondrial health, and the cumulative impact of vaccines administered in infancy.
4. Acknowledge and Investigate Subpopulation Risks
Averaging data across millions obscures those few but real individuals who suffer serious adverse events.
Ethical science demands that public health authorities not merely acknowledge, but proactively seek to understand which groups (based on genetics, immune status, prior injury, etc.) face elevated vaccine risks.
Research into vaccine response variability, mitochondrial disease markers, immune dysregulation syndromes, and epigenetic susceptibilities must be accelerated. Informed consent requires that patients be told not only the average risk but also if they may fall into a vulnerable group.
Precision vaccination must replace one-size-fits-all public health policy.
5. Communicate with Intellectual Honesty and Humility
Public trust is eroded not by transparency about uncertainty, but by its absence. Medical and public health authorities must stop treating any acknowledgment of risk or complexity as dangerous. True scientists welcome scrutiny; dogmatists fear it.
The willingness to openly admit gaps in knowledge, to describe competing hypotheses, and to engage respectfully with critics is not weakness—it is strength.
A culture of intellectual honesty, not authoritarian messaging, will win back skeptical parents, doctors, and citizens.
Conclusion
Vaccines are one of the most widely used medical interventions in the world—and unlike most medical treatments, they are administered prophylactically to otherwise healthy individuals.
This extraordinary context demands an equally extraordinary safety standard. In a society that upholds ethical medicine, any product given preemptively to healthy people must meet the strictest bar for proven benefit and minimal harm.
Anything less is a violation of the core medical principle: First, do no harm.
Each instance of vaccine injury must be treated not as an unfortunate inevitability to be quietly ignored, but as a sentinel event demanding the full investigative resources of public health.
Every serious adverse outcome following vaccination should be studied with the same rigor, urgency, and seriousness we would devote to a hospital error or a contaminated drug batch. Each case must serve as a learning opportunity to improve vaccine design, screening for vulnerabilities, and risk mitigation strategies.
Unless vaccine safety is made the foremost priority—ahead of public relations goals, ahead of programmatic vaccine coverage targets, ahead of corporate interests—vaccine skepticism and hesitancy will inevitably continue to grow.
No amount of public messaging campaigns can substitute for true safety improvements. People intuitively understand when concerns are dismissed rather than answered. In a free society, skepticism is not a problem to be eradicated—it is a safeguard of science and public ethics.
It is only by radically recommitting to transparency, humility, scientific rigor, and ethical responsibility that public health institutions can truly rebuild trust. And it is only by holding vaccines to the highest possible safety standard that we can honor both the public good and the individual dignity of every person we aim to protect.